Economy Minister Akmal Nasrullah Mohd Nasir at the launch of Targeted SDG Bersasar Programme 2026. PHOTO: IRDA
The invitation arrived unexpectedly. I hadn’t planned a trip to Batu Pahat, but it had been years since my last visit. Curious to see what had changed, I decided to make the journey.
The bus from Johor Bahru cost RM20 and took just over two hours. When I arrived, I asked several people for directions to Dataran Penggaram. They looked puzzled. It turned out they knew the place—just not by its official name.
Dataran Penggaram, the public square where the launch was held. PHOTO: CHUAH BEE KIM
I had come to Batu Pahat for the launch of the Targeted SDG Bersasar Programme 2026. Rather than rolling out another nationwide programme using a one-size-fits-all approach, the government wants each district to focus on the issues most relevant to its own community.
The programme was organised by the Economy Ministry together with state and local partners, including the Iskandar Regional Development Authority (IRDA), the Johor government and local authorities.
In his speech, Economy Minister Akmal Nasrullah Mohd Nasir said national policies could no longer be implemented through a one-size-fits-all approach. District-level interventions, he said, should be shaped by local challenges and opportunities.
He also reminded the audience that Malaysia has less than four years left to meet its 2030 Sustainable Development Goals.
Akmal also spoke about the Johor-Singapore Special Economic Zone (JS-SEZ), describing it as a catalyst for high-value investment, advanced industries, regional supply chains, local talent development and skilled employment.
The JS-SEZ covers 11 key sectors, from manufacturing and logistics to healthcare, education and the digital economy. It aims to attract 50 projects within five years and 100 within a decade, while creating 20,000 skilled jobs.
But what caught my attention wasn’t just the scale of those ambitions. It was the minister’s emphasis that their benefits should extend beyond Johor’s traditional growth areas.
“The spillover benefits from JS-SEZ are expected to extend across the Southern Region, including Batu Pahat, Muar, Pontian and Kluang, through stronger local enterprises, supply chains, logistics, agro-food, tourism and digital economy activities,” he said.
Listening to him, I found myself wondering about a different question.
Why Batu Pahat?
At first glance, Batu Pahat might seem an unusual choice. The district performs well across many development indicators. Poverty and unemployment are relatively low, while access to water, electricity and secondary education is almost universal.
Yet one statistic stood out.
Maternal mortality.
In 2024, Batu Pahat recorded a poverty rate of 2.4 per cent and an unemployment rate of 1.3 per cent. It had full access to water and electricity, while its upper-secondary education completion rate stood at 98.1 per cent.
However, its maternal mortality ratio was 52.1 deaths per 100,000 live births—well above Johor’s 33.3 and the national figure of 24.3.
“Our goal is not merely to understand statistics. Our goal is to ensure more mothers receive timely care and return safely to their families,” Akmal said.
The programme’s targeted outcomes include mapping maternal and child healthcare services, improving delivery processes, reducing bureaucratic barriers, encouraging collaboration between communities and frontline workers, and establishing mechanisms to monitor progress and measure real-world impact.
The participants at the launch. PHOTO: IRDA
After the launch, there was a brief press conference. That, however, is a story for another day.
For now, Kingston Hotel 25 offered a comfortable place to rest before I caught the bus back to Johor Bahru the next morning.
A night at the Kingston Hotel 25 @Summit Signature Batu Pahat. PHOTO: CHUAH BEE KIMBatu Pahat Express Bus Terminal, where I began my journey home to Johor Bahru. PHOTO: CHUAH BEE KIM
My trip was brief. There wasn’t enough time to visit Pantai Minyak Beku or wander through the older parts of town. Those will have to wait for another visit.
Sometimes accepting an invitation leads to a story you didn’t expect to find. Batu Pahat turned out to be one of those places.
Hannah Yeoh, Minister in the Prime Minister’s Department (Federal Territories), meets mothers of children with Type 1 diabetes at Kampung Orang Asli Sungai Temon (Seletar). PHOTO: CHUAH BEE KIM
Under a tent at an evening community gathering in Johor Bahru, a small group of mothers sat down with Minister in the Prime Minister’s Department Hannah Yeoh to talk about children living with Type 1 diabetes.
Their concerns were practical and urgent. They included access to diabetes technology, school support, public awareness, and the daily burden of keeping a child safe.
Yeoh listened attentively and said she would raise the matter with the Health Ministry.
It was a small, unscripted moment — plastic chairs, a community gathering, not a press conference.
But for the mothers, being heard mattered.
Type 1 diabetes, or T1D, is a lifelong autoimmune condition. It is not caused by diet or lifestyle, is not preventable, and currently has no cure. Children with T1D need insulin to survive, but managing the condition goes far beyond injections.
Families have to monitor blood glucose levels, count carbohydrates, calculate insulin doses, adjust for meals and physical activity, and remain alert to medical emergencies every day.
For parents, that responsibility does not stop when a child goes to school, joins a sports activity or even at bedtime.
K. Kanageswary was among the mothers present.
She used to work as a security officer in Singapore, but when her daughter was diagnosed with T1D three years ago, she had to leave that job to care for her.
“When I was working in Singapore, I had to leave my house at 4.30am and would only be back home at around 10.30pm,” she later shared with me.
“My daughter’s condition needed me to take care of her, so I quit the job and found a job in Johor Bahru which gives me more time to care for her, but the salary is a challenge for someone managing her condition.”
For Kanageswary, practical assistance would make a difference.
“It would really help if the government could help by distributing vouchers for buying relevant medical supplies,” she said.
The financial burden can be heavy for families managing T1D.
In a paper prepared by Frederick Yap’s mother and shared with me, families highlighted the cost of blood glucose test strips, ketone strips, needles, Continuous Glucose Monitoring sensors, insulin pump consumables and emergency glucose supplies. The paper also noted that an insulin pump can cost about RM30,000, while CGM-related costs may range from hundreds to a few thousand ringgit a month, depending on the system and supplies used.
The mothers also raised the need for better school-based support.
Children with T1D may need to eat, drink water, check their glucose levels, take insulin or rest when their blood sugar is out of range. But when teachers or school staff are unfamiliar with the condition, these needs can be misunderstood.
This is why awareness matters.
A child asking for a snack may not be seeking special treatment.
A child who suddenly looks tired, emotional or unfocused may not be misbehaving.
A child who needs to pause may simply be trying to stay safe.
For families living with T1D, support is not only about hospital appointments. It is also about classrooms, sports fields, tuition centres and community spaces understanding what the condition requires.
Kampung Orang Asli Sungai Temon, a Seletar fishing community facing growing pressure from coastal development, pollution and declining fishing grounds. PHOTO: CHUAH BEE KIM
The setting itself had its own story
Yeoh met the mothers at Kampung Orang Asli Sungai Temon, a Seletar fishing community. The kampung is no stranger to outside visits. Volunteers from Pertubuhan Kebajikan Pelita JB have worked with Cornerstone International School to bring education support to children in the community.
It is one small, steady effort in a kampung still facing a much longer struggle over land, pollution and a fishing livelihood increasingly squeezed by coastal development.
That evening, two different concerns shared the same space.
One was about an indigenous fishing community trying to protect its home and way of life.
The other was about mothers trying to protect children living with a lifelong medical condition.
Both were asking for the same basic thing: to be seen, heard and supported in practical ways.
For the mothers of children with T1D, Yeoh’s willingness to listen was not the end of the journey.
But it was a start.
And for families who live with the condition every day, even a start matters.
Ice cream for the kids of Kampung Sungai Temon, handed out by Yeoh. PHOTO: CHUAH BEE KIM
Frederick Yap (left) with his teammates, coaches, and supporters after a school football tournament in Johor Bahru. PHOTO: FALCON KNIGHT UNITED FC
When Frederick Yap first joined Falcon Knight United FC in 2022, his coach did not see Type 1 diabetes.
He saw a cheerful, positive child who was relentless when chasing the ball.
He saw a good defensive player.
“Honestly, it was a surprise to me, as Frederick is always the most energetic one,” said the coach.
That surprise matters.
Type 1 diabetes is not caused by diet or lifestyle. It is not preventable, and there is currently no cure. Children living with the condition need insulin to survive, but managing it goes far beyond injections.
Every day, families have to monitor blood glucose levels, count carbohydrates, calculate insulin doses, adjust for meals and physical activity, and stay alert for emergencies.
On a football pitch, that means the adults around a child need to know when something is not right.
“We have adjusted to have more awareness and attention to Frederick’s behaviour,” the coach said.
He now watches not just Frederick’s movement on the field, but also his expression and behaviour. A sudden change could mean that Frederick’s blood sugar is too low or too high, and that he needs attention.
That is not the same as treating him as fragile.
Frederick’s parents do not want him to be pitied. They want him to be accepted, supported and allowed to participate like other children.
This is where the coach’s role becomes important.
A child who needs water, food, a glucose check, insulin, or a short rest is not being difficult. He may simply be doing what is necessary to stay safe.
A child who suddenly looks tired, emotional or less focused may not be misbehaving. His blood sugar may be out of range.
The need for awareness goes beyond one football team. In a paper prepared by Frederick’s mother and shared with me, she noted that children with T1D can face challenges in school because many educators remain unfamiliar with the condition.
This can lead to misunderstandings during low-blood-sugar episodes, or restrictions on essential self-care activities such as eating, drinking water, checking blood glucose or taking insulin.
The same awareness is needed in sports clubs.
Children do not leave Type 1 diabetes at home when they go to school, tuition, football training or a tournament. Their condition follows them into every classroom, field and changing room.
At Hospital Sultanah Aminah in Johor Bahru alone, about 70 children and adolescents are being followed for Type 1 diabetes care. That number may sound small, but for each family, the responsibility is constant.
The financial burden is also heavy. The paper noted that an insulin pump can cost about RM30,000, while CGM systems may cost anywhere from RM600 to RM2,500 a month, depending on the system and supplies used.
Technology can help. But awareness still matters.
A sensor can alert a family. A parent can carry supplies. A child can learn to speak up.
But in the moment, the adult standing closest to the child — a teacher, coach, trainer or organiser — may be the person who notices first.
That is why Frederick’s coach supports more awareness and training.
He has also worked with players with autism and severe attention-deficit hyperactivity disorder (ADHD).
“We have always given our best, because football is for everybody,” he said.
For this coach, inclusion is not a slogan. It is something that happens in small decisions.
Letting a parent step in when needed.
Watching a child more closely without embarrassing him.
Understanding that support is not special treatment.
Allowing a child to pause, recover and return.
Frederick’s story is not only about football. It is about what happens when the adults around a child are willing to learn.
His coach did not know at first.
Then he watched Frederick play.
And now he watches differently.
Not with pity. With awareness.
That may be the first step towards making more schools, clubs and community spaces safer for children living with Type 1 diabetes.
Because childhood should not stop at diagnosis.
And football, as the coach said, is for everybody.
The children who love football, after a tournament where Frederick and his teammates finished fourth. PHOTO: FALCON KNIGHT UNITED FC
Frederick’s dream of returning to football came true when his team finished fourth in a friendly tournament organised by Johore Chinese Football Association for schools state-wide. PHOTO: FALCON KNIGHT UNITED FC
On a football pitch in Johor Bahru, Frederick Yap had a job to do.
Playing defensive midfield, he stood just in front of the defenders, where the work is not always glamorous but almost always important. His role was to pressure, disrupt, track advancing opponents and break up attacks before they became dangerous.
It was a position that demanded stamina, strength, composure and positional intelligence.
For Frederick, it was also something more.
The nine-year-old was returning to the pitch after almost two years away, having been diagnosed with Type 1 diabetes in April 2024. He had stopped training and playing immediately after his diagnosis. But according to his parents, his natural sporting ability had not disappeared.
Football was not new to him. Neither was movement. He had always shown a flair for physical activities, from football to skateboarding, picking things up quickly and fearlessly.
To anyone watching from the side, he may have looked like any other active, bright and determined child on the field.
But for his parents, the match was never just a match.
It was also glucose levels, insulin, snacks, hydration, ice packs, emergency supplies and the constant calculation that comes with caring for a child whose blood sugar can change within minutes.
His mother put it plainly: “Type 1 diabetes does not take a break.”
That sentence stayed with me.
Because childhood should be allowed to run. It should be allowed to sweat, compete, laugh, fall, get back up and try again. But for families living with Type 1 diabetes, every ordinary activity carries an extra layer of planning.
Before the tournament, Frederick’s parents had to think about what many parents never have to consider. Would he have enough snacks in case his glucose dropped? Would there be enough fluids to keep him hydrated? How would they keep his insulin cool under the hot sun? How would his body respond to intense activity?
Exercise can make the body more sensitive to insulin and cause glucose to be used up faster. For a child with Type 1 diabetes, that means sports can sometimes cause blood sugar to rise or fall unexpectedly. Even after exercise, insulin sensitivity may remain elevated for several hours, raising the risk of night-time lows.
So his parents prepared.
They carried snacks. They carried insulin. They carried glucose. They monitored his levels. They watched for signs. They calculated, adjusted and stayed alert.
At one point during the two-day tournament, keeping the insulin cool under the hot sun became such a concern that the family had to drive to a nearby 7-Eleven to buy a whole bag of ice.
The ice was meant for the insulin.
By the end of the day, it had become useful for the children too. Other young players came over asking for ice cubes to cool down their bodies and drinks.
It was a small scene, but it said a lot.
Sometimes care looks like a parent standing quietly at the sidelines. Sometimes it looks like a bag of ice. Sometimes it looks like planning so carefully that a child gets to feel like every other child.
That, perhaps, is the heart of Frederick’s story.
His parents do not want him to be treated as fragile. They do not want pity. They do not want his condition to become the first thing people see.
They want him to be accepted, supported and understood.
During the tournament, only the coaches were aware of his condition. His teammates did not necessarily know. To them, he was simply Frederick — a boy who loved football and wanted to play.
The coaches allowed his parents to step into the dugout when needed to check his glucose level through a continuous glucose monitor (CGM). Apart from that, he was judged by the same things that matter in sport: performance, character, attitude and effort.
That kind of support matters.
Not because children with Type 1 diabetes need to be wrapped in cotton wool, but because they need adults around them to understand what the condition requires.
There were difficult moments. His family said there were times when Frederick had to stop playing because his blood sugar was too low or too high. For a parent, it is heartbreaking to watch your child sit out while teammates continue.
But it is also necessary.
The challenge is not only physical. It is emotional too. A child has to learn that taking a short break does not mean he is weak. It does not mean he has failed his team. It is simply part of living with Type 1 diabetes.
And each time Frederick returned to the field, he showed something important: with preparation, support and determination, children with Type 1 diabetes can still take part in sports and chase their goals.
His team finished fourth.
But the more meaningful achievement may not have been the placing. It was the return.
It was a child stepping back onto the field after a diagnosis that could easily have frightened a family into saying no. It was parents choosing not to let fear become a cage. It was a reminder that illness may change the way a family plans, but it should not be allowed to take away a child’s right to play.
Still, Frederick’s story also raises a wider question.
How much of this burden should families have to carry alone?
His parents believe there is still not enough awareness about Type 1 diabetes in schools and the wider community. Many people still do not understand that Type 1 diabetes is an autoimmune condition. It is not caused by eating too much sugar. It is not contagious. Children with Type 1 diabetes are not naughty, weak or difficult. They simply need insulin to survive and support to manage their blood glucose safely.
Frederick’s family is not alone in this. But just how many Malaysian families share this experience? The numbers are not easy to pin down.
A BERNAMA commentary by consultant physician, endocrinologist and diabetologist Dr Chooi Kheng Chiew, citing the Ministry of Health’s National Diabetes Registry Report 2023, said 289 individuals under 18 were recorded as living with diabetes in Malaysia. The same commentary noted that paediatric cases, especially Type 1 diabetes, are often not captured in adult-focused systems, which means the real number is likely higher. It also cited International Diabetes Federation data stating that 977 Malaysian children and teenagers under 18 had been diagnosed with diabetes—a figure that includes both Type 1 and Type 2 cases.
For families like Frederick’s, the data gap matters. If children with Type 1 diabetes are not clearly seen in the numbers, their needs may also be less visible in schools, sports and public support systems.
For some families, the gaps in support are not just inconvenient—they are exhausting. What would it look like if Malaysia had a dedicated foundation for Type 1 diabetes? Not just a charity that writes cheques, but one that builds systems: training for teachers, subsidies for CGMs, and a community for families who often feel they are managing this alone.
Access is not only about awareness. It is also about continuity of supplies, affordability and the tools families need to manage the condition safely.
This is where the conversation becomes bigger than one football match.
Malaysia does not lack diabetes awareness entirely. But Type 1 diabetes in children is specific enough, misunderstood enough and demanding enough that families may need a clearer platform of support — especially when it comes to schools, sports, CGM access and public understanding.
For schools, the needs are not complicated, but they are important.
Teachers and coaches should know the signs of low and high blood sugar. They should understand why a child may need to drink water, go to the toilet, eat a snack, check glucose levels or rest for a while. They should know that a child who cannot concentrate may not be misbehaving. His blood sugar may simply be out of range.
Classmates and other parents also need awareness.
A child should not be teased for wearing a CGM. He should not be made to feel strange for taking insulin or eating during class when medically necessary. He should not be excluded from sports or activities because the adults around him are unsure what to do.
Understanding does not mean lowering expectations.
It means making participation safer.
It means allowing a child to be a child.
For some families, managing T1D can cost hundreds of ringgit a month. Frederick’s parents said the financial burden rises sharply for those who rely on diabetes technology. An insulin pump can cost about RM30,000 upfront, while CGM sensors can cost about RM600 a month. With tubing and related supplies, they estimate that the first-year cost for a child using both an insulin pump and CGM can approach RM50,000. The recurring cost may be lower after the initial pump purchase, but sensors and consumables still need to be replaced regularly.
Frederick’s message to other children with Type 1 diabetes is simple: “Don’t be afraid. You’re not alone.”
It is the kind of sentence adults would do well to take seriously.
Because children should not have to be brave alone. Their parents should not have to educate every room from scratch. Schools should not wait for an emergency before learning what Type 1 diabetes means.
What families like Frederick’s need is not sympathy. They need a clearer support system.
For some, that could mean a dedicated Type 1 Diabetes foundation — one that advocates for CGM access, trains teachers and coaches, and connects families so no one has to navigate this alone.
A support system would not remove the burden of Type 1 diabetes. But it could ensure that preparation and understanding are not left to chance.
Because a child’s safety on the field should not depend only on what his parents remember to pack.
It should also depend on the adults around him knowing what to do.
Most of all, it should allow him to play.
Author’s note: The family featured in this story has given permission for their experience to be shared. Some details have been included with their consent. The data cited from the Ministry of Health and International Diabetes Federation is accurate as of the time of writing.
Frederick’s dream of returning to football came true when his team finished fourth in a friendly tournament organised by the Johore Chinese Football Association. PHOTO: FALCON KNIGHT UNITED FC
A misplaced phone in a car became a small reminder that not every human problem fits neatly into an automated system. IMAGE: AI-GENERATED ILLUSTRATION VIA CHATGPT
A young lawyer once told me she preferred not to deal with people.
At the time, I found it funny. Perhaps even understandable. Anyone who has worked with clients, customers, bosses, suppliers or service counters will know that human beings can be wonderfully complicated creatures.
But lately, I have been thinking about the other side of that statement.
What happens when we need a human being — and the system gives us an app, a chatbot or a help page instead?
I got into a Grab car recently and noticed a handphone on the seat. The driver, flustered, remembered his last passengers — a woman and her elderly mother, whom he had fetched from a clinic.
He took a small detour to check if they were still nearby. They were not. He said he would return after dropping me off.
What struck me was not just his effort. It was what he said next: there used to be a support line he could call for situations like this. Now everything is automated. He did not know who to contact.
The story ended well. The phone owner eventually called.
But what if she had not?
The second story did not end as cleanly.
A travel app showed a limited-time offer — last two rooms, timer running. After I entered my bank details, the cursor kept spinning. Uncertain whether the payment had gone through, I tried again.
It had.
I had made a double booking.
I immediately tried to cancel one. The bot said it could be cancelled but not refunded — policy. When I tried to explain what had happened, it replied: “I do not understand your issue.”
A bot acting like a bot is forgivable.
The next day, I contacted the app company, the hotel and the bank.
The app company said it would look into the matter and check with the hotel. The bank said it could not do anything as the issue was between me and the app company. The hotel understood perfectly, but said the app company would have to handle it.
About a week later, the app company sent an email stating that it would cancel the booking because I had changed my mind. I replied that I had not changed my mind, and explained once again what had happened.
Another email, signed by another person, arrived in my inbox saying he would look into it. Then came a third email, from yet another person, saying the booking could be cancelled but the money would remain in the app for me to use on another booking. In other words, the booking could be cancelled, but the payment would not be returned to me as a refund.
I was not cancelling the trip. I was requesting that one unnecessary booking be reversed because the booking process had failed at a critical moment. There is a difference between offering store credit and taking responsibility for what went wrong.
That, to me, is the real problem. Not automation itself, but automation without human accountability.
Apps are useful when everything goes according to script. But when the script breaks, someone still has to take ownership, exercise judgement and decide what is fair.
A company can spend heavily on branding and promotions to attract customers. But when something goes wrong, can it also respond with basic goodwill instead of hiding behind process?
This is the gap that automation has not closed.
Not routine transactions. Apps handle those well enough.
But moments that require judgement, context and the ability to say: “I understand what happened, and I am going to help make this right.”
Is automation useful? Of course.
Until something unexpected surfaces — something that needs empathy, discretion or simply a person willing to listen.
Apps can be automated. Processes can be automated. But accountability cannot be automated away.
Some problems still need a human voice. The irony is that the more systems try to remove that voice, the more valuable it becomes.
Note: Images used in this post are AI-generated illustrations created with ChatGPT.
The Apple Store at the Exchange TRX in Kuala Lumpur. PHOTO: CHUAH BEE KIM
During five hours at Apple The Exchange TRX in Kuala Lumpur, I watched people buy premium technology almost as casually as they might order a cup of coffee.
It was a weekday, but the store hummed with a weekend crowd. Perhaps the mid-year school holidays explained part of it. Still, what struck me was not merely the number of people inside Malaysia’s first Apple Store.
It was the way many of them appeared to shop.
Customers approached staff with questions and requests. Some seemed ready to make their purchases without needing lengthy persuasion. The staff were not chasing reluctant shoppers or running through aggressive sales pitches. The buyers were already curious. Some looked as though they had arrived already convinced.
The products seemed to sell themselves.
I was there for a simple data transfer between my old phone and my new one. With five hours to kill, I became a quiet observer of this retail ecosystem.
The staff were undeniably impressive. Despite the relentless foot traffic, those I encountered were composed, patient and pleasant.
But the real force in the room was not the service. It was the invisible pull of the brand itself.
That pull became clearer when I thought back to my Grab ride to the mall earlier that day.
The driver had shared a painful chapter of his life. Driven by a passion for cooking, he had once invested a substantial amount in a restaurant business.
It did not last. Eventually, he faced the hard truth that pouring more money into the venture was merely funding a sinking ship. He chose to cut his losses and walk away.
Later in the ride, he spoke about a local omakase operator whose business, he said, was thriving.
The contrast stayed with me. Here was one man with culinary skills, raw passion and substantial capital whose business did not survive, while another appeared to thrive in one of the most premium segments of the dining market.
The driver believed branding had made a difference. His own bak kut teh venture, he said, had started with only a small allocation for branding.
Naturally, reality is more complicated. A single conversation during a Grab ride does not reveal the whole truth. Factors such as location, rent, pricing, margins, timing and operational execution could all have shaped the outcome. It would be unfair to draw a definitive conclusion from one person’s account.
Yet, sitting in the Apple Store hours later, his words echoed.
Why do some businesses have to work so hard for every single ringgit, while others appear to attract premium buyers with far less resistance?
A bak kut teh dish competes on taste, portion size, price and familiarity. It satisfies a daily hunger.
Omakase sells something different. Beyond the food, it offers curation, craftsmanship, exclusivity and experience.
Similarly, Apple is not merely selling a phone, a tablet or a laptop. It is selling design, familiarity, an ecosystem and the confidence many customers attach to its name.
Branding cannot rescue a bad product. Nor does a sleek logo guarantee commercial success.
But a good product is merely the baseline.
Before customers reach for their wallets, they must first be given a reason to desire what is being sold.
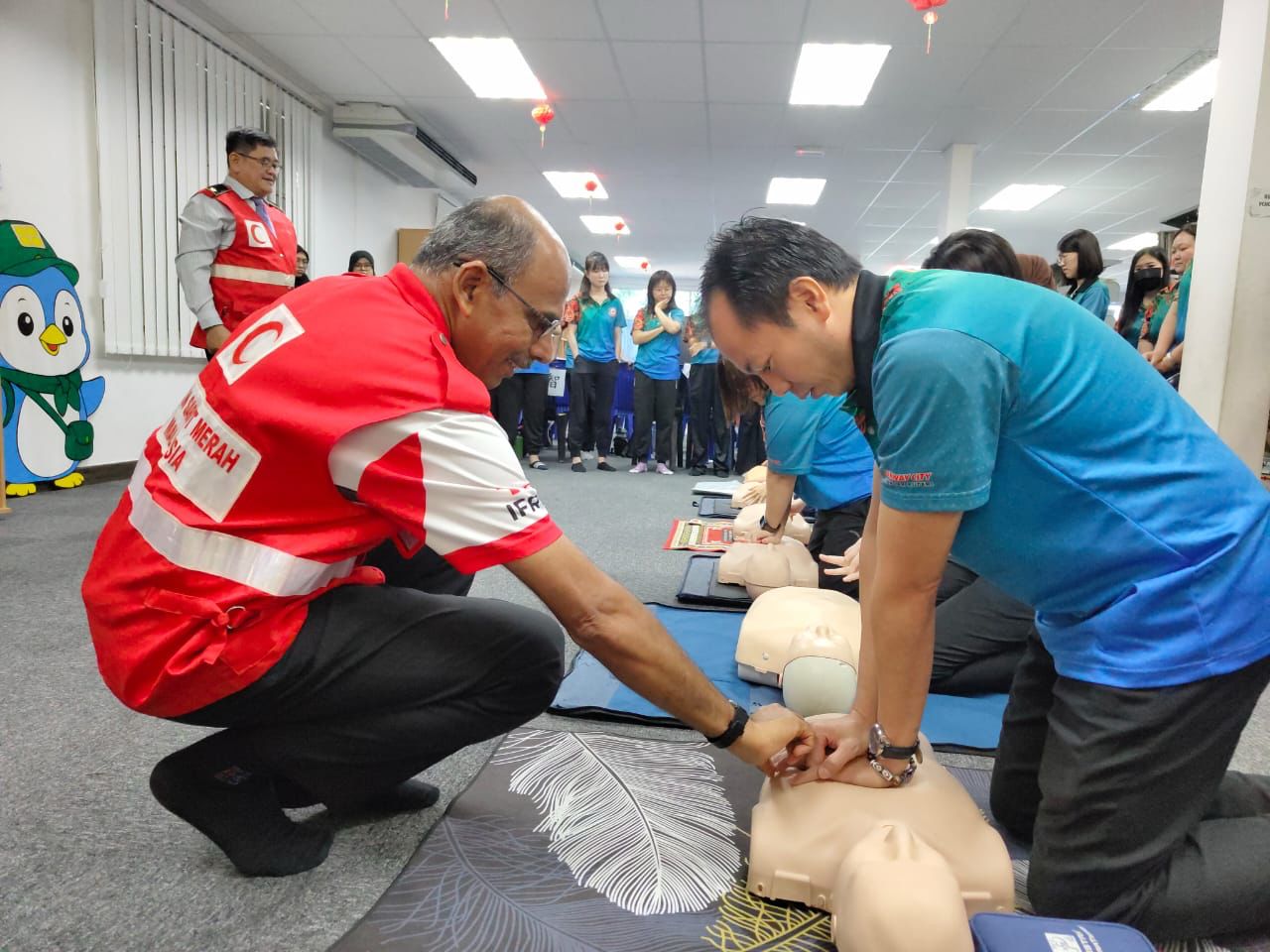
Khoo Jet Seng, Honorary Secretary of the Malaysian Red Crescent Society Johor Bahru Branch, during the CPR and AED training session at SJK(C) Cheah Fah in Iskandar Puteri. The school’s headmaster, Ing Boon Keong, is seated on the far left. PHOTO: LEE WEE KIONG.
There is a cabinet near the entrance of my regular mall. I walk past it sometimes. It says AED above it — Automated External Defibrillator — with a red heart and a lightning bolt symbol that signals something urgent. I assume the device is inside.
I have never seen anyone open it.
I have also never checked whether the battery inside still works, whether the pads have expired, or whether anyone in the vicinity is actually trained to use it. I suspect most people who walk past it haven’t either.
This is not a criticism of the mall. Malaysia has been moving — rightly — toward wider AED placement in public spaces, with Selangor studying guidelines for new developments and public areas.
But here is the question I keep turning over: what about schools?
A child spends roughly six hours a day, five days a week, at school. Teachers are, by sheer daily proximity, the adults most likely to be present if a student collapses — whether from sudden cardiac arrest, a medical episode, or something nobody saw coming. And yet there is no equivalent mandate requiring AEDs in Malaysian schools. No policy. No allocation. The gap is not from a lack of caring. It is, honestly, a matter of money.
A single AED unit can cost several thousand ringgit, with some Malaysian suppliers placing typical prices roughly between RM5,000 and RM15,000, depending on the model and features. Then there is the maintenance — battery replacements, pad expiry, servicing — which adds up quietly over time. For most government schools operating on tight budgets, this is not a realistic line item. So the machines don’t come.
And here is where it gets uncomfortable: even where AEDs do exist — in malls, in lobbies, along highways — I wonder how many of us would actually reach for one. Panic is a strange thing. In a real emergency, the three seconds of knowing where the device is and the thirty seconds of remembering how to use it can feel very far away from any training session you may have attended two years ago. Muscle memory requires repetition. Most of us have had none.
Koh Yee Mei, Rotary Club of Tebrau project organiser, Lee Wee Kiong, Training Officer-in-Charge of the Malaysian Red Crescent Society Johor Bahru Branch, taking part in the CPR and AED training programme at SJK(C) Cheah Fah in Iskandar Puteri. PHOTO: LEE LIE FEEI.
The gap is not entirely about equipment. It is also about whether people know what to do in the minutes before help arrives.
This is why I found myself paying attention when I came across what the Rotary Club of Tebrau (RCT) has been doing quietly in Johor Bahru.
Rather than waiting for the AED funding question to resolve itself — which could take years — they are building the human infrastructure first. Since 2023, in partnership with the Malaysian Red Crescent Society Johor Bahru branch, they have been training teachers and school staff in CPR and AED use. Not a one-off event. A rolling programme, school by school, batch by batch. The most recent sessions were held at Sekolah Jenis Kebangsaan (Cina) Cheah Fah in Iskandar Puteri.
The logic is straightforward and, I think, rather wise.
An AED without a trained person nearby is just a box on the wall. But a trained person — someone who knows what to do, how to stay calm, and how to act in those first critical minutes — is already a first responder, with or without the machine.
If the machine eventually arrives, they will know how to use it. If it does not arrive yet, they are still better equipped than they were yesterday.
Dr A.R. Leenah Devi Rajah, who leads the RCT, put it plainly: “One minute of first aid can change a life, especially in a school setting where teachers spend the most time with students on a daily basis.” Teachers are the adults in the room. Training them is the most practical place to start.
I will admit I came to this story as an outsider. I am not a medical professional. I cannot tell you whether the AED in your mall lobby is in working condition, or who is responsible for checking it, or whether your school’s canteen aunty has ever done a CPR course. These are questions I genuinely do not know the answer to — and I suspect they are questions most of us have never thought to ask.
What I do know is this: cardiac arrest does not wait for the right location. It does not check whether you are in a mall, a classroom or a school field. And in Malaysia, where cardiovascular disease (CVD) is affecting people at younger ages — with the National Heart Institute (IJN) citing a 2019 study that found almost one in four CVD patients were below 50 — the odds that a teacher, a staff member, or a fellow student might one day need to act are not as remote as we would like to think.
The RCT cannot solve the whole problem alone. But it is doing something concrete, in a place where children spend most of their waking hours, with the people most likely to be standing there when it matters.
Participants, organisers and trainers gather for a group photo following the CPR and AED training session held at SJK(C) Cheah Fah. PHOTO: ROTARY CLUB OF TEBRAU
All photos courtesy of Rotary Club of Tebrau and Koh Yee Mei, the event organising chairperson and project organiser.
The news report on the CPR and AED training programme at SJK(C) Cheah Fah in Iskandar Puteri is on Newswav.